If You Oppose ObamaCare You’re RAAAAACIST and UNEDUCATED!!
- 0share
- Share
- Tweet
- Comment Now 0
Cross-posted from American Power.
*****
Out of the blue, I got this on Twitter earlier this morning:
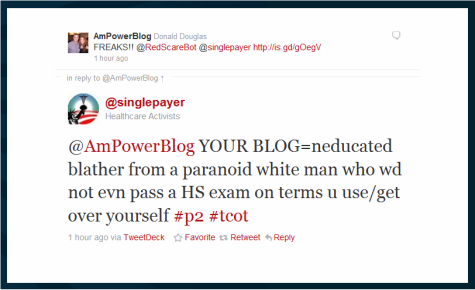
I replied here.
@SinglePlayer then blocked me, typical for a leftist totalitarian.
RELATED: At Doug Ross, “New England Journal of Medicine Inadvertently Hands House GOP the Game Plan for Starving ObamaCare.” If you can’t completely kill it (at first), squeeze funding until implementation becomes impossible:
The ACA contains 64 specific authorizations to spend up to $105.6 billion and 51 general authorizations to spend “such sums as are necessary” over the period between 2010 and 2019. None of these funds will flow, however, unless Congress enacts specific appropriation bills. In addition, section 1005 of the ACA appropriated $1 billion to support the cost of implementation in the Department of Health and Human Services (DHHS)…. [and the] ACA appropriated nothing for the Internal Revenue Service, which must collect the information needed to compute subsidies and pay them. The ACA also provides unlimited funding for grants to states to support the creation of health insurance exchanges (section 1311). But states will also incur substantially increased administrative costs to enroll millions of newly eligible Medicaid beneficiaries…
Without large additional appropriations, implementation will be crippled.
And thank goodness. That would be like a symphony.
See Dr. Marc Siegel, “ObamaCare Will Clog America’s Medical System“:
ObamaCare was lauded by many for covering all Americans with pre-existing conditions. That’s not the issue. We’re going to get into trouble because of the kinds of coverage that the new law mandates. There are no brakes on the system. Co-pays and deductibles will be kept low, and preventive services will have no co-pays at all. That sounds like a good deal for patients, yes? But without at least a pause to consider necessity and/or cost, expect waiting times to increase, ERs to be clogged and longer lead times needed to make an appointment.
Patients with new Medicaid cards who can’t find a doctor will go where? To emergency rooms. The escalating costs of these visits (necessary and unnecessary) will be transferred directly to the American public, both in the form of taxes as well as escalating insurance premiums.
Beginning in 2014, insurance exchanges will be set up in every state so that individuals can choose a health insurance plan. This will help control costs, right? Wrong. Don’t expect to find individually tailored plans or those with higher deductibles or co-pays. They won’t be there because they can’t receive the government stamp of approval.
In the new system, my patients will be able to see me as often as they’d like. But will they get the same level of care? I don’t think so. I anticipate that more expensive chemotherapies and cardiac stents or transplants, for instance, will have a tougher time being approved, as is already the case in Canada.
Over on the public side, the new Independent Payment Advisory Board – established by the health reform law to “recommend proposals to limit Medicare spending growth” – will advise Medicare that some treatments are more essential and more cost-effective than others. I believe that value judgments inevitably will have to be made, reducing my options as a practicing physician. Private insurers will follow suit, as they often do.
During the battle over this reform, you often heard, even from President Obama, that you’d be able to keep the plan you have. What he didn’t say – but what we now know – is that because of this new law, the private markets will have to remake their plans, that the costs will rise and that the plan you were told you could “keep” is in all likelihood no longer available. But when your plan changes, backers of reform will simply blame it on those evil private insurance companies.
The truth is, private health insurance is a low-profit industry, with profit margins of 4% compared with over 20% for major drug manufacturers. With the additional costs of no lifetime caps and no exclusion for pre-existing conditions, these companies will be compelled to raise their premiums in order to stay in business. The individual mandate is supposed to be the tradeoff by providing millions of new customers, but there is no guarantee that this additional volume will preserve profits with all the new regulations. This is what occurred in New York state in 1992, when a new law denied exclusion on the basis of pre-existing conditions.
Clogged emergency rooms, death-panel rationing, and reduced consumer choice.
That’s what @SinglePayer is all about.
*****
More great blogging at American Power.
- 0share
- Share
- Tweet
- Comment Now 0






